Multiple Sclerosis
Multiple Sclerosis: Understanding, Managing, and Living Well
What Is Multiple Sclerosis?
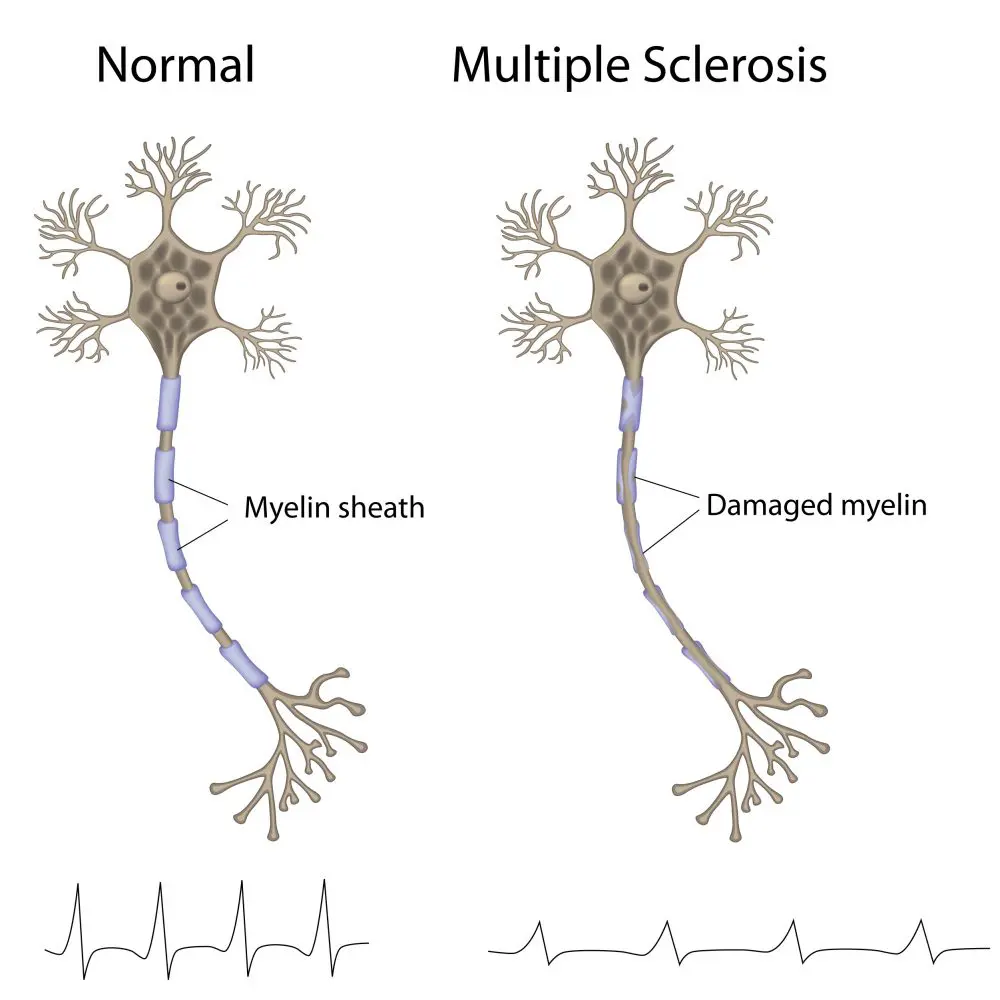
Multiple sclerosis (MS) is a chronic neurological disease in which the immune system attacks myelin—the protective coating around nerve fibers in the brain and spinal cord. This damage disrupts communication between the brain and the body. The good news? Modern disease-modifying therapies (DMTs) can slow disease progression, reduce relapses, and help most people maintain function and quality of life for decades.
According to WebMD, MS affects roughly 2.3 million people worldwide and typically strikes people between ages 20-40, though it can occur at any age. It’s more common in women—affecting them 2-3 times more than men.
Think of MS like your immune system’s “friendly fire”—it mistakenly targets and attacks the protective coating of your nerves, causing communication breakdowns between your brain and body. This damage can affect vision, movement, sensation, and many other functions.
The MS Process: What Happens in Your Body
Myelin and Nerve Communication
Understanding MS requires understanding myelin:
| Component | Function |
|---|---|
| Myelin | Protective insulating sheath around nerve fibers |
| Purpose | Allows rapid electrical signal transmission along nerves |
| Damage in MS | Immune cells attack and destroy myelin (demyelination) |
| Result | Signals travel slowly or become blocked |
| Plaques/Lesions | Scarred areas where myelin was destroyed |
Inflammatory Cascade
In MS, the immune system becomes dysregulated and attacks myelin-producing cells. This creates a cycle of inflammation, demyelination, and nerve damage that progressively affects multiple areas of the nervous system (“multiple sclerosis” = “multiple scars”).
Types of Multiple Sclerosis
MS presents in different patterns, each requiring different management approaches.
Relapsing-Remitting MS (RRMS) — Most Common
| Feature | Details |
|---|---|
| Prevalence | 80-85% of people at diagnosis |
| Pattern | Defined relapses (attacks) followed by remissions |
| Relapse | New symptoms or return of old symptoms lasting 24+ hours |
| Duration | Relapses last days to weeks to months |
| Recovery | Complete or partial recovery (remission) |
| Progression | May transition to SPMS within 10 years (50% of patients) |
| Female Predominance | 2:1 ratio (women more commonly affected) |
Relapse Management:
According to PMC research, when relapses occur:
High-dose IV methylprednisolone (MP) is first-line treatment
Treatment should start within days of relapse onset for best results
IV-MP 1g/day for 3-5 days is standard protocol
Most patients show significant improvement with early treatment
Primary Progressive MS (PPMS)
| Feature | Details |
|---|---|
| Prevalence | 10-20% of people at diagnosis |
| Pattern | Steady worsening from disease onset |
| Relapses | Absent—no distinct relapses or remissions |
| Progression | Gradual disability accumulation |
| Characteristics | More aggressive, higher axonal loss |
| Challenge | Fewer treatment options available |
Secondary Progressive MS (SPMS)
| Feature | Details |
|---|---|
| Development | Develops in ~50% of RRMS patients within 10 years |
| Pattern | Steady progression with/without superimposed relapses |
| Transition Point | Usually after 10-20 years of RRMS |
| Disability | Progressive, stepwise worsening |
| Mechanism | Transition from inflammatory to neurodegenerative |
Progressive-Relapsing MS (PRMS) — Rarest
Steady progression from onset
Occasional relapses superimposed
Affects <5% of MS patients
Symptoms: Wide-Ranging and Variable
MS symptoms vary dramatically depending on which nerves are damaged. Symptoms can appear suddenly or gradually.
Common Motor Symptoms
✓ Movement and Muscle Control:
Weakness or paralysis (often one side of body)
Spasticity (muscle stiffness and involuntary contractions)
Tremor or coordination problems
Difficulty walking or balance issues
✓ Vision and Eye Problems:
Blurred or double vision
Optic neuritis (eye nerve inflammation)
Eye pain with movement
Loss of color vision
Sensory and Neurological Symptoms
✓ Sensation Changes:
Numbness or tingling (often first symptom)
Burning sensations
Electric shock feelings (Lhermitte’s sign)
Pain
✓ Cognitive and Emotional:
Brain fog or difficulty concentrating
Memory problems
Depression or mood changes
Anxiety
Emotional lability (unpredictable mood swings)
Autonomic Symptoms
✓ Body Function Control:
Bladder problems (urgency, frequency, retention)
Bowel difficulties (constipation, incontinence)
Sexual dysfunction
Abnormal sweating
Fatigue (most common, most disabling symptom)
Diagnosis: A Multi-Step Process
Diagnostic Criteria
MS diagnosis requires evidence of dissemination in space and time — meaning lesions in multiple locations affecting the nervous system at different times.
Diagnostic Tests
MRI (Magnetic Resonance Imaging) — Gold Standard
According to classic MS diagnostic research, MRI is the best method for demonstrating dissemination in space:
Shows brain and spinal cord lesions clearly
Detects lesions in 72% of MS patients vs. 55% with other tests
Reveals active inflammation (contrast-enhancing lesions)
Shows chronic damage (T1 “black holes”)
Most sensitive and specific test for MS
| MRI Finding | What It Means |
|---|---|
| Active Lesions | Enhance with contrast; ongoing inflammation |
| Chronic Lesions | T2 hyperintense areas; old demyelination |
| T1 Black Holes | Severe tissue damage with axonal loss |
| Location | Periventricular, juxtacortical, infratentorial sites |
Evoked Potentials (EP)
Studies show EPs help diagnose MS, especially when MRI is normal or when assessing specific pathways:
Visual evoked potential (VEP) — optic nerve function
Brainstem auditory evoked response (BAER) — brainstem involvement
Somatosensory evoked potential (SSEP) — spinal cord function
CSF (Cerebrospinal Fluid) Analysis
Oligoclonal bands — IgG abnormalities in MS
Elevated immunoglobulin levels
Pleocytosis (elevated white cells)
Clinical Examination:
Neurological assessment
Documentation of symptoms and their timeline
Assessment of dissemination in space and time
Treatment: Multiple Approaches
Disease-Modifying Therapies (DMTs)
According to recent treatment reviews, all DMTs for relapsing forms of MS reduce CNS immune-mediated inflammation, improving clinical and radiologic outcomes.
Interferon Beta — First-Line Therapy
Interferon beta (IFNβ) was the first DMT and remains a standard treatment:
| Interferon Type | Mechanism |
|---|---|
| How It Works | Increases anti-inflammatory cytokines; decreases pro-inflammatory ones |
| Proven Benefit | Reduces relapse rates 25-35% |
| Lesion Reduction | Decreases MRI brain lesions significantly |
| Disability Impact | Delays progression of disability |
| Administration | Subcutaneous or intramuscular injection |
| Long-Term Safety | Excellent safety profile over decades |
Other DMT Classes Available:
Monoclonal antibodies (e.g., natalizumab, ocrelizumab)
S1P receptor modulators (fingolimod, siponimod)
Oral small molecule drugs (dimethyl fumarate, teriflunomide)
Newer agents with diverse mechanisms
DMT Selection Factors:
MS type (RRMS vs. PPMS)
Disease activity (relapses, MRI lesions)
Individual patient factors (tolerability, comorbidities, pregnancy plans)
Disease severity
Relapse Management
According to evidence-based treatment guidelines:
Acute Relapse Treatment:
IV Methylprednisolone (IV-MP): 1g daily for 3-5 days
First-line therapy for moderate-to-severe relapses
Timing critical: Start within days of symptom onset for optimal benefit
Shortens relapse duration and may improve recovery
Additional Considerations:
Oral corticosteroid taper after IV treatment (individualized)
Treatment can be started as late as 1-2 months into relapse
Earlier treatment generally produces better outcomes
Symptom Management
Fatigue (Most Common Symptom):
Rehabilitation and exercise programs
Medication (amantadine, methylphenidate)
Pacing and energy management
Treatment of sleep disorders
Spasticity:
Physical therapy and stretching
Baclofen, tizanidine, or other muscle relaxants
Botulinum toxin for localized spasticity
Other Symptoms:
Vision problems: Corticosteroids for optic neuritis, vitamin B12 supplementation
Pain: Neuropathic pain medications, physical therapy
Cognitive issues: Cognitive rehabilitation, computerized training
Mood disorders: Antidepressants, counseling
Rehabilitation and Physical Therapy
According to comprehensive reviews, structured rehabilitation significantly improves outcomes:
Evidence-Based Benefits:
| Intervention Type | Benefits Demonstrated |
|---|---|
| Exercise Programs | Improve muscle strength, endurance, mobility |
| Physical Therapy | Enhance functional capacity, reduce fall risk |
| Walking Programs | Critical for maintaining independence and quality of life |
| Balance Training | Improve proprioception, prevent falls |
| Multidisciplinary PT | Longer-term gains in activity and participation |
Specific Recommendations:
Regular moderate-intensity aerobic exercise
Resistance training 2-3 times weekly
Balance and coordination exercises
Flexibility and stretching programs
Living With MS: Stages and Quality of Life
Four Stages of MS Progression
| Stage | Characteristics |
|---|---|
| Initial (Diagnosis) | Recent diagnosis, understanding condition, starting treatment |
| Early | Little disability, good functional status |
| Later | Moderate disability developing, more symptom impact |
| Advanced | Severe disability, significant mobility/function loss |
Important Note: 20-30% of MS patients never develop major disabilities even 20+ years after diagnosis with proper treatment.
Quality of Life Management
Multidisciplinary Approach:
Regular neurologist follow-up
Physical therapy and rehabilitation
Occupational therapy for daily living adaptation
Psychological counseling and support
Social support and patient advocacy groups
Vocational counseling if work-related issues arise
Frequently Asked Questions
MS itself is rarely directly life-threatening. However, severe relapses, complications, or advanced disability can affect life expectancy if untreated. With modern DMTs and proper management, most people with MS have normal or near-normal life expectancy.
Currently, no cure exists. However, modern disease-modifying therapies can control disease activity remarkably well in many patients, sometimes achieving a state of “no evidence of disease activity” (NEDA).
Yes. Without DMTs, MS typically progresses. Most RRMS patients develop SPMS within 10 years if untreated. DMTs significantly reduce relapse rates, MRI lesions, and disability progression.
MS progression varies greatly between individuals. Some have mild symptoms and slow progression; others experience rapid worsening. With early treatment, progression slows considerably.
Many people with MS continue working successfully, especially with treatment and accommodations. Some may need to adjust work schedules or tasks. Cognitive symptoms or fatigue can affect work capacity in some cases.
Common triggers include infections, stress, lack of sleep, and heat. While avoiding all triggers is impossible, recognizing personal triggers helps manage disease activity.
MS has genetic predisposition but is not directly inherited. Having a parent with MS increases risk but doesn’t guarantee development. Multiple genes and environmental factors contribute.
Modern DMTs have dramatically improved MS prognosis. Many patients achieve low disease activity. Quality of life is often good with proper management, rehabilitation, and support systems in place.
Your Next Steps with NeuroLogic Neurocare
Dr. Mohammed Imran Khan specializes in diagnosing and managing multiple sclerosis. Early diagnosis and prompt initiation of disease-modifying therapy significantly improve long-term outcomes and quality of life.
Quick Links:
Early diagnosis and treatment matter. With modern disease-modifying therapies, most people with MS can control their disease and maintain excellent quality of life. Contact NeuroLogic Neurocare today to get a comprehensive evaluation, accurate diagnosis, and start effective treatment. Your future with MS can be very positive with proper care.
Disclaimer:
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. If you’re experiencing symptoms suggestive of MS (vision problems, numbness, weakness, balance issues), consult a qualified neurologist for proper evaluation and personalized treatment recommendations. Always discuss your symptoms, diagnostic findings, and treatment options with your healthcare provider.