Paralysis
Paralysis: Understanding, Recovery, and Living Independently
What Is Paralysis?
Paralysis is the loss of muscle function in one or more body parts, usually resulting from nerve damage that disrupts communication between the brain and muscles. The good news? Many forms of paralysis can improve significantly with intensive rehabilitation and modern neuroplasticity-based therapies. Recovery is often possible even in severe cases.
According to Cleveland Clinic, paralysis results when something disrupts nerve signals to your muscles, preventing voluntary movement. The two most common causes are strokes and spinal cord injuries, though paralysis can result from many other conditions.
Think of paralysis like a broken communication line between your brain and muscles. The signal can’t get through, so the muscles don’t move. However, research shows the brain can rewire itself and find new pathways—a process called neuroplasticity—allowing recovery that was once considered impossible.
Types of Paralysis: Understanding the Distinctions
Paralysis Classification by Location
| Type | What It Affects | Details |
|---|---|---|
| Monoplegia | One limb (arm or leg) | Often from stroke or nerve injury |
| Hemiplegia | One entire side of body (arm, leg, face) | Common after stroke |
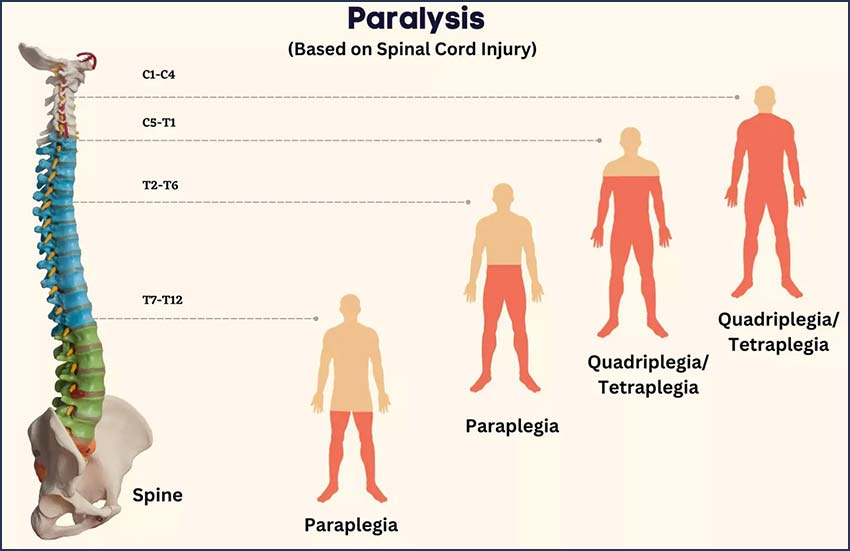
| Paraplegia | Both legs (spinal cord injury at T1-L5) | Arm function preserved |
| Tetraplegia | All four limbs (spinal cord injury at C1-T1) | Also called quadriplegia |
| Diplegia | Both limbs on one side (rare) | Usually from brain injury |
Paralysis by Severity
| Classification | Movement Ability |
|---|---|
| Complete | No voluntary movement below injury level |
| Incomplete | Some voluntary movement preserved |
| Flaccid | Muscles are floppy and weak |
| Spastic | Muscles are stiff with involuntary contractions |
Common Causes of Paralysis
Traumatic Causes (Sudden Injury)
According to WHO, traumatic spinal cord injuries are the leading cause:
Spinal Cord Injury:
Falls – Most common traumatic cause
Road traffic accidents – Second leading cause
Violence – Including penetrating injuries
Sports injuries – From impacts or falls
Work-related accidents – Occupational injuries
Brain Injury/Stroke:
Ischemic stroke – Blood clot blocks blood flow
Hemorrhagic stroke – Bleeding in brain
Head trauma – Traumatic brain injury
Non-Traumatic Causes
According to WHO, non-traumatic causes are increasing, especially in aging populations:
Spinal tumors – Cancerous or benign
Degenerative conditions – Disc herniation, stenosis
Vascular conditions – Aortic dissection, aneurysm
Infections – Spinal infections causing inflammation
Autoimmune diseases – MS, transverse myelitis
Toxins and medications – Toxic exposure or drug side effects
Birth defects – Spina bifida, tethered spinal cord
Secondary Complications from Paralysis
Paralysis affects more than just movement—it impacts entire body systems:
✓ Respiratory:
Breathing difficulties if respiratory muscles affected
Aspiration risk (food entering airways)
✓ Urinary and Bowel:
Loss of bladder and bowel control
Increased infection risk
✓ Circulatory:
Deep vein thrombosis (blood clots)
Orthostatic hypotension (dizziness with position change)
✓ Skin:
Pressure ulcers (bedsores)
Increased infection risk
✓ Musculoskeletal:
Muscle atrophy and contractures
Bone loss and osteoporosis
Diagnosis: Identifying Type and Severity
Clinical Assessment
According to rehabilitation experts, diagnosis involves:
Neurological Examination:
Muscle strength testing (0-5 grading scale)
Reflexes and muscle tone
Sensation testing
Coordination and balance
Cranial nerve function
ASIA Impairment Scale:
Used to classify spinal cord injury severity from A (complete) to E (normal function)
Diagnostic Tests
| Test | Purpose |
|---|---|
| MRI Scan | Detailed imaging of brain and spinal cord |
| CT Scan | Quick imaging, especially for acute trauma |
| X-Rays | Identifies bone fractures and alignment issues |
| Nerve Conduction Studies | Measures how fast nerves send electrical signals |
| EMG (Electromyography) | Evaluates muscle and nerve function |
| Blood Tests | Detects infections or autoimmune conditions |
Recovery Through Neuroplasticity: The New Understanding
What Is Neuroplasticity?
According to recent research, neuroplasticity is the brain’s ability to reorganize and form new neural connections—essentially rewiring itself after injury.
This changes everything: Previous thinking held that spinal cord injury meant permanent paralysis. Modern neuroplasticity research shows recovery is possible even in severe cases through intensive therapy.
How Neuroplasticity Works in Paralysis Recovery
According to comprehensive research, several mechanisms enable recovery:
| Mechanism | How It Works |
|---|---|
| Cortical Remapping | Brain reassigns functions to undamaged areas |
| Synaptic Strengthening | Remaining nerve connections reinforced through repetition |
| Collateral Pathways | Alternative neural routes formed around damaged areas |
| Neurogenesis | New nerve cells generated in brain and spinal cord |
| Structural Plasticity | Physical brain reorganization and remodeling |
Key Finding: Repetition Is Essential
Neuroplasticity research consistently shows that intensive, task-specific physical training for several hours daily drives the most recovery. The more a person practices specific movements, the more the brain relearns control.
Why This Works:
Repeated stimulation strengthens remaining neural pathways
Brain learns new movement patterns
Even incomplete injuries have many preserved connections to work with
Treatment and Rehabilitation Approaches
Acute Phase Management
Immediate Care (First Hours/Days):
Immobilization to prevent further damage
Medical management (steroids, medication)
Airway and breathing support if needed
Monitoring for complications
Intensive Rehabilitation: The Key to Recovery
According to evidence, rehabilitation focusing on neuroplasticity principles drives recovery:
Physical Therapy Components:
| Approach | Details |
|---|---|
| Active Exercises | Patient moves affected limbs (when possible) |
| Passive Movement | Therapist moves limbs to stimulate nervous system |
| Task-Specific Training | Practice of functional movements (reaching, stepping) |
| Intensive Dosage | Several hours daily for maximum neuroplastic effect |
| Progression | Gradually increasing difficulty and independence |
Advanced Rehabilitation Technologies
Modern technology enhances neuroplasticity-based recovery:
Robotic-Assisted Therapy:
Brain learns from assisted movement patterns
Intensity and precision optimize neuroplastic learning
Functional Electrical Stimulation (FES):
Electrical impulses activate paralyzed muscles
Can restore some voluntary movement with practice
Interactive Metronome (IM):
Uses visual cues and rhythmic beats to retrain brain-body coordination
Synchronizes movement with visual and auditory rhythm
Improves coordination and motor control
Transcranial Magnetic Stimulation (TMS):
Non-invasive brain stimulation to encourage neuroplastic changes
Activates specific brain regions involved in recovery
Epidural Stimulation:
Electrodes placed near spinal cord
Electrical stimulation combined with rehabilitation
Specific Rehabilitation Exercises
According to stroke rehabilitation specialists, structured exercises drive recovery:
Lower Body Exercises:
Ankle pumps – Move feet up and down (improves circulation)
Toe raises – Elevate toes while heels stay down
Heel slides – Slide heels along floor toward body
Leg lifts – Raise leg against gravity
Knee bends – Controlled knee flexion
Hip bridges – Lift hips from lying position
Upper Body Exercises:
Shoulder raises – Lift arms out to sides
Arm reaches – Extend arms forward and sideways
Grip exercises – Strengthen hand and finger muscles
Rotation – Rotate torso gently
Balance and Coordination:
Heel-to-toe walking – Test balance and coordination
Sit-to-stand transitions – Functional movement
Weight shifting – Improve balance awareness
Cardiovascular:
Walking (with assistive devices if needed)
Stationary cycling (motorized or assisted)
Arm ergometry – Upper body aerobic activity
Assistive Technology and Devices
Daily Living Aids
According to WHO, assistive devices dramatically improve independence and quality of life:
Mobility Devices:
Wheelchairs (manual and powered)
Walkers, canes, crutches
Orthotic braces and supports
Scooters for longer distances
Home Modifications:
Portable ramps for thresholds
Grab bars and railings
Raised toilet seats and shower chairs
Accessible kitchen setup
Self-Care Aids:
Long-reach grabbers
Adaptive utensils and cups
Button hooks and sock aids
Adapted clothing
Emerging Technologies
The future holds promising assistive innovations:
Robotic Exoskeletons:
Wearable powered devices enabling standing and walking
Some allow independent ambulation with training
Improve cardiovascular health and psychological well-being
Brain-Computer Interfaces (BCIs):
Neural signals decoded to control external devices
Emerging technology for commanding prosthetics or exoskeletons
Represents future of paralysis recovery
Smart Home Technology:
Voice-controlled systems
Automated lighting and temperature
Smart locks and security
Improve independence and safety
Living With Paralysis: Quality of Life and Independence
Multidisciplinary Support Team
Optimal recovery requires coordination among multiple specialists:
✓ Neurologist – Diagnosis and medical management
✓ Physical Therapist – Rehabilitation and movement training
✓ Occupational Therapist – Adaptive strategies for daily living
✓ Psychology/Counseling – Emotional support and adaptation
✓ Social Worker – Resources and community support
✓ Nursing – Ongoing care and complication prevention
✓ Vocational Counselor – Work and employment planning
Psychological Adjustment
Paralysis profoundly affects emotional well-being:
Common Emotional Responses:
Depression and grief
Anxiety about future
Loss of identity and role
Anger and frustration
Supports That Help:
Counseling and therapy
Support groups with others
Peer mentors (those further along in recovery)
Family involvement and education
Long-Term Outlook
Research shows neuroplasticity continues enabling recovery for years, not just months after injury:
Some recovery possible years after injury
Intensive therapy remains effective at any stage
Technology continues advancing rehabilitation options
Many people achieve surprising functional recovery
Frequently Asked Questions
Many forms of paralysis can improve significantly or even resolve with intensive rehabilitation, especially incomplete paralysis. Complete paralysis recovery is more limited but possible to varying degrees with neuroplasticity-based therapies. Research continues expanding what’s achievable.
Initial intensive rehabilitation typically occurs over months to years. However, neuroplasticity research shows recovery continues for years after injury. Early intensive therapy shows the best results, but therapy at any stage can produce improvement.
Depends on the cause, severity, and whether the injury is complete. Some regain most function, especially with stroke. Spinal cord injury recovery is more variable but often exceeds expectations with intensive therapy and emerging technologies.
Recovery varies greatly by cause:
Stroke: 20-30% show significant motor improvement
Spinal cord injury: Variable; incomplete injuries have better prognosis
Other causes: Depends on underlying condition
Yes. While complete spinal cord injury historically meant permanent paralysis, emerging therapies, emerging technologies, and neuroplasticity research show partial recovery is possible in many cases. Research into new treatments continues.
Neuroplasticity is the foundation for all paralysis recovery. It’s the brain’s ability to rewire itself and form new neural pathways, compensating for damaged ones. Intensive, repetitive rehabilitation optimizes this process.
Early rehabilitation (within hours to days) produces the best outcomes. However, recovery remains possible even years later through neuroplasticity. Early start is important but never “too late” to begin.
Assistive devices enable independence, improve function, and support rehabilitation. Advanced technologies like robotic assistants and brain-computer interfaces are revolutionizing paralysis management.
Your Next Steps with NeuroLogic Neurocare
Dr. Mohammed Imran Khan specializes in diagnosing and managing paralysis, coordinating comprehensive rehabilitation approaches. Early expert evaluation and intensive therapy initiation significantly improve recovery outcomes.
Quick Links:
Recovery is possible. Neuroplasticity research shows the brain can rewire itself and regain function. With intensive rehabilitation, modern technologies, and expert guidance, remarkable recovery is achievable even from severe paralysis. Contact NeuroLogic Neurocare today to start your recovery journey. Time is critical—early intensive rehabilitation produces the best outcomes.
Disclaimer:
This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. If you’re experiencing paralysis or loss of movement, seek immediate medical attention for proper evaluation and emergency care. Always consult a qualified neurologist or medical specialist for personalized diagnosis, treatment recommendations, and rehabilitation planning.